“All domination is, in the last instance, maintained through social control strategies”
(Bonilla-Silva 2001:25)
The moment I learned the identity of the shooter behind the Aurora massacre (read white male), I knew how the story would go. James Holmes would immediately be subjected to amateur psychiatric diagnoses — he would be “sick”, “insane”, “sociopathic”. I imagined headlines just like this — “What Does a Killer Think? Is the Colorado shooter delusional, depressed, or psychotic? And how do we stop the next one?”
His story would be his lonesome own, no matter that he precisely shared the demographic characteristics of the vast majority of the 56 other mass murderers/spree killers who have shot up schools and malls and workplaces over the past 30 years.
But the true power of this story becomes clear in juxtaposition of competing systems of social control — the Medicalization of White versus the Criminalization of Black/Brown.
A conversation with a colleague (one with whom I have had frequent chats with about the construction of the school to prison pipeline ) brought the point home.
“You know, I never fully understood what you were talking about until I saw the coverage of Aurora and then thought about what they did to Trayvon”, she said.”Five minutes after we knew the Colorado shooters identity, he was described as mentally ill and…”
“And Trayvon was criminalized even though he was the victim, even though he was the one who was actually dead??” I interjected.
“Yes” she replied sadly. “There it was.”
White Privilege, Deviance and Social Control
Certainly one of the prime benefits of white privilege is the right to represent yourself and to do so without fear that your actions will be used to condemn all who look like you. Or vice versa.
Chancey DeVaga sums it up perfectly:
When viewed through the white racial frame, there is nothing in his deeds on last Friday night that reflects upon the behavior of white people, generally, or white men in particular…..
The freedom to kill, maim, commit wanton acts of violence, and to be anti-social (as well as pathological) without having your actions reflect on your own racial group, is one of the ultimate, if not in fact most potent, examples of White Privilege in post civil rights era America. Instead of a national conversation where we reflect on what has gone wrong with young white men in our society–a group which apparently possesses a high propensity for committing acts of mass violence–James Holmes will be framed as an outlier.
But the power of white privilege extends beyond individual versus collective accountability and representation. The white racial frame also shapes the labels we attach to aberrant white behavior and the systems we call upon to control the related deviance. Although James Holmes is indeed facing criminal charges of the most extreme sort, it is the medical model that is called on to “understand” him. He isn’t totally “bad” — despite his horrific criminal acts, Holmes is a mutant, an aberration on the trajectory of “normal” white maleness. Even in the context of criminal justice – insanity pleas or no, death penalty or no — he will be viewed as “psychopathic”, ultimately then as “sick”. Someone should have/could have “helped” him before it was too late. Of course, one of the key features of the medical model involves mitigating deviant behavior by attributing it to “sickness rather than badness”, with a particular focus on the condition rather than the behavior and treatment as opposed to punishment.
The white racial frame increasingly sees white “deviants” as sick – and maybe some are — but contrast this with the framing of both offenders and victims of color. They are irredeemably “evil” — no questions asked, guilt assumed, and punishment — in draconian legal systems not posh private treatment centers — is the corresponding response. The collective taint of criminalization is so strong that the actually innocent may be easily swept up, wild racial hoaxes furthered without sufficient doubt, and victims, such as Trayvon Martin, reframed via” white logic” as dangerous hoodie-wearing thugs who ultimately got just what they deserved.
Deviance, “Discretion” and Double-Standards
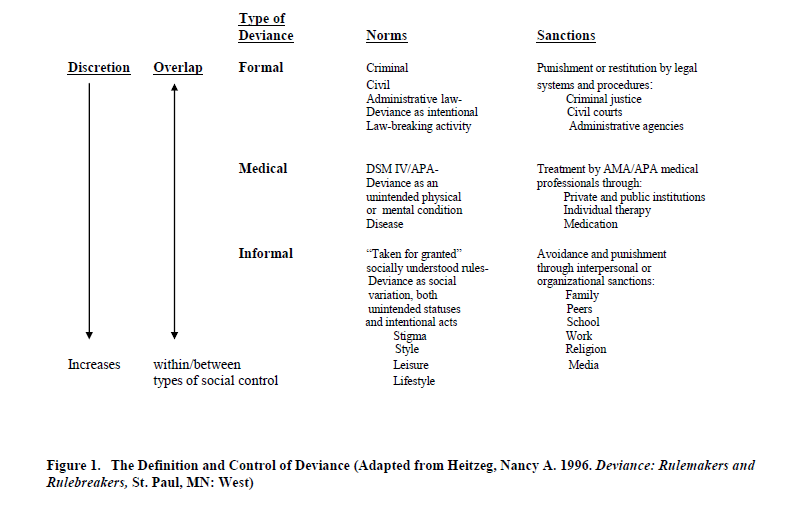
The labeling of “deviants” offers informal/extra-legal, medical and formal/legal options, all designed, at least in theory to regulate particular types of rule-breaking. (See Figure 1). Informal, medical and formal systems of social control all involve varying degrees of discretion or flexibility in decision-making, as to who should be controlled and how. These models suggest that different types of deviant behavior warrant different types of social control; i.e. minor deviations may be handled via highly discretionary informal social control, deviants who have mental illnesses may best be served by the “expert” judgment and treatment of the medical model, and intentional violators of the law must be punished via formalized legal systems.

A closer examination of the mechanisms of social control, however, reveals that the type of social control exerted has much less to do with the deviation in question and much more to do with the demographics of the deviant. Far from being mutually exclusive or race and class blind, these systems of control are inter-dependent and over-lapping, and discretion often is shaped by discrimination.
Race, class and gender are inextricably bound up with the definition and control of deviance. To the extent that the privileged and empowered “norm” is white, male, financially well off, heterosexual and adult, then people of color, women, the poor, GLBT persons, and the young become “the Other“, the “abnormal”, the “deviant”.
Further, these “Others” have been subject to labeling and social control based on the intersection of race, class, gender and other differences. The “matrix of domination” shapes access to systems of social control as well as to social opportunity. And, while there are “deviants” of all classes, all races, all genders and ages, the models under which they are controlled reflect their relative social status. The informal markers and sometime associated stigmas of race, class and gender often provide the foundation for escalations in social control, leading to medicalization of the “redeemable” white middle and upper classes and criminalization for the poor and communities of color.
Indeed, the medical model and criminal justice have operated as parallel systems for comparable deviations but disparate deviants from the outset. The medical model was always a therapeutic alternative for whites, women and the well-to do, while crime has long “been imputed to color”. Analysts have argued that the very foundations of criminal justice are rooted in racism and classism, that in fact our notions of crime and criminal justice have essentially served the primary function of social control of persons of color and the poor. While these disparities are long standing, in recent years, two key trajectories have magnified the disparities in these systems of control – the inter-connected rise of both the medicalization of deviance and the prison industrial complex.
Medicalization versus Prisonization
Once laden with stigma and images of the publicly funded insane asylum, the treatment of mental illness is now a multi-billion dollar industry, privatized and driven by the wide-spread use of pharmaceuticals to treat nearly every major affliction. Let’s just call it the Medical Industrial Complex. The medical model is based in an understanding of deviance as individual “sickness”, i.e. psychological or physical “abnormalities create a deviant condition. The medical model largely denies social and structural factors and focuses attention instead on treatment of the mind and body of the “deviant”. Hence the long list of Mental Disorders outlined in the American Psychiatric Associations'(APA) Diagnostic and Statistical Manual of Mental Disorders (DSM) lists symptoms devoid of social context.
While psychiatric labels carry their own disadvantages, they certainly are most often preferable to the sanctions laid out by the criminal justice system. The medical model offers the deviant the shelter of the “sick role” and an exception from certain responsibilities, save compliance with treatment. Increasingly in an era of mass advertizing for pharmaceuticals, potential patients are encouraged to self-diagnosis and then “ask their doctor” for the meds they need to wake up, fall asleep, cheer up, get it up, leave the house, do their homework and so on.
Access to this model requires insurance or sufficient wealth to accommodate psychiatrists, $50,000 stays at private treatment facilities, and psychotropic medications. The expansion of the model was initially sparked by the privatization of the addiction treatment industry for Substance Use Disorders, and now extends far beyond.
One of the major growth sectors of psychiatry is the diagnosis and treatment of Disorders of Infancy, Childhood and Adolescence (DICA), particularly the Disruptive Behavior Disorders of Attention-Deficit Hyperactivity Disorder, Oppositional Defiant Disorder and Conduct Disorder. These diagnoses are widely used in the context of K-12 and beyond:
In 2003, six million American schoolchildren—about 15 percent—took methlphenidate (Ritalin) alone. Methylphenidate has replaced Prozac as the drug defining an entire cohort, with authors beginning to speak of a “Ritalin nation,” a “generation Ritalin,” and the like.
Students themselves actively seek the ADHD diagnosis. The pills have many uses related to the spectacularized culture of testing, overwork, stress, and body-consciousness—they aid in concentration, provide wakefulness, suppress appetite, assuage certain emotions, and improve athletic performance. They can be crushed and snorted or smoked recreationally in ways similar to methamphetamines. The diagnosis itself directly addresses high-stakes testing: medicated or not, ADD and ADHD-diagnosed students can request additional time in many testing circumstances.
Many more students than diagnosed use the medication: There is an active black market in Ritalin in every educational environment from primary school through graduate degrees. Students pay up to $10 a dose for “vitamin R.”
These psychiatric labels perfectly overlap with potential educational and legal labels, and thus offer an alternative mechanism for parents, school officials and law enforcement to deal with disciplinary infractions and drug use by both adults and juveniles.(See Figure 2) Indeed, research indicates that class, insurance coverage, and race are key indicators of who receives treatment. These factors play a significant role in the labeling of youth in particular; study after study shows racial disparities in the diagnosis and treatment of ADHD as well as other Disruptive Behavior Disorders, with the indication that teachers were most likely to expect and define ADHD as an issue for white boys.
The expansion of the medical model creates new opportunities for the diversion of white and middle-class children and adults from the juvenile and criminal justice systems. Their substance use, their disruptive behavior, their deviance may now be defined as an addiction and a disease, not as a disciplinary infraction or a crime. White deviance is mitigated as “disease”. And as a bonus, the medical industrial complex makes billions pushing prescription drugs to children and their parents and offering them expensive treatment once they are addicted to the same.

From Nancy A. Heitzeg, “Race, Class and Legal Risk in the United States: Youth of Color and Colluding Systems of Social Control”Forum on Public Policy, Oxford University Press, Winter 2009.
The existence of a therapeutic medical alternative also makes the rise of the punitive state of juvenile and adult criminal justice possible. It allows for the harsh mandatory prison terms associated with the War on Drugs aka The New Jim Crow — there is now a safety value for diverting the white, the well- to -do, the celebrity into treatment. It allows for the increasing punitive penalties associated with both educational systems and juvenile justice; it makes the school to prison pipeline possible with little fear of ensnaring white middle class youth. It allows for the mass incarceration of millions of people of color without the concomitant risk of targeting privileged race and class groups. The rise of the medical model creates the context for the escalating risks for youth and adults of color by insuring that their white counter-parts may not be caught in the same legal net. And it allows some to say, even in the face of the horrible crimes of Aurora and elsewhere, that a white mass murder’s actions must be mitigated – not only by the individualistic perks of white privilege – by appeals to mental illness and diminished responsibility.
Shaking Off the White Racial Frame
Back to where we started — James Holmes and Trayvon Martin. I hope the absurdity is clear but let me say it plain. What kind of racialized double-standards allow a young white male to purchase thousands of dollars of assault weapons, tactical gear, ammunition and explosive materials unchecked, unnoticed while a young black male is targeted for Walking While Black?? What sort of white denial seeks an immediate medical mitigation for a shooter who kills 12 and wounds 70 while idling avoiding the victimization of a young man executed by a vigilante? Or worse yet, denying it all together by entertaining the notion that it was somehow deserved because he was a “gangster” or :::shudder::: wearing a hoodie??
Of course James Holmes and Trayvon Martin are but two cases, but they illustrate the general trend. People of color are disproportionately – no overwhelming criminalized via informal media-driven stigma and stereotypes, by racial profiling, by a white racial frame that assumes guilt and demands suspension/expulsion, imprisonment, execution. Conversely their white counter-parts, who use drugs — legal and otherwise – at a comparable rate, commit white on white violence/white on black violence, organized sexual assaults and in fact, the vast majority of all crime, are exceptionalized, individualized, and, dare i say it ?? at least partially excused by appeals to the medical model. So much for “the safety and security” crowd and their concern for “crime”.
In America, folks often ask, “what the hell is wrong with black people?” In the aftermath of the Colorado Movie Massacre, Columbine, and many other incidents, we need to ask, “what the hell is wrong with young white men?
Sadly, that question will not be asked on a national stage. White privilege is blinding. In the case of James Holmes, it also mutes a much needed national conversation about the ties between (white) masculinity and violence.
Let me be clear. I am not calling for increased criminalization of white people. CI stands for Abolition, and calls for transformative justice as an alternative to mass incarceration. Nor am I suggesting that the psychiatry does not have a place — just that the current over-diagnosis driven pharmacological soup does not. Our current systems of social control have failed to make us safer or saner and in fact, both the medical industrial complex and the prison industrial complex are just soaking our fears and insecurities, appealing to/upholding white privilege for massive profit. That is what they are intended to do — dope us up, lock us up, divide up us, cha-ching!!
White privilege has its’ costs as well as benefits, and the racism that under-pins it, is taking a toll. We are looking for trouble in all the wrong places, relying on racialized profit-driven systems to regulate “deviants” within a white male racial frame. The notion that we can identify “deviants” by their race, their class their attire, the notion that we can police or pill-pop our way to safety and security without any analysis of the social structural factors that may correlate with “deviance”, now that is the real insanity.
Years ago, before pseudo-suave serial killer Ted Bundy was to be executed, he was granted a last TV interview (Yes let’s talk about white male privilege) where he blamed his rape/murder sprees on alcohol and hard core pornography. A medicalized mitigation, “addictions”, he called them. The next day in various classes — didn’t matter which classes – students could not stop talking about it. The conversation always went like this – lots of questions about his mental health, discussions about the links between pornography and sexual violence, the role of alcohol and inhibition, lots of anger, but even more confusion. And the last comment — barely audible, indeed a whisper – was always this:
“But he seemed so normal.”
Exactly. And that is the entire point..
Shake off the racial fog — it’s costing us, killing us all.
Join us in defending the truth before it’s too late
The future of independent journalism is uncertain, and the consequences of losing it are too grave to ignore. To ensure Truthout remains safe, strong, and free, we need to raise $46,000 in the next 7 days. Every dollar raised goes directly toward the costs of producing news you can trust.
Please give what you can — because by supporting us with a tax-deductible donation, you’re not just preserving a source of news, you’re helping to safeguard what’s left of our democracy.